Bicalutamide was patented in 1982 and approved for medical use in 1995.[35] It is on the World Health Organization's List of Essential Medicines.[36] Bicalutamide is available as a generic medication.[37] The drug is sold in more than 80 countries, including most developed countries.[38][39][40] It was at one time the most widely used antiandrogen in the treatment of prostate cancer, with millions of men with the disease having been prescribed it.[23][41][42][43][44] Although bicalutamide is also used for other indications besides prostate cancer, the vast majority of prescriptions appear to be for treatment of prostate cancer.[44]
In Japan, bicalutamide is uniquely used at a dosage of 80 mg/day both in combination with castration and as a monotherapy in the treatment of prostate cancer.[48][49]
Bicalutamide is also employed for the following off-label (non-approved) indications:
To reduce the effects of the testosterone flare at the initiation of GnRH agonist therapy in men[50][51]
Bicalutamide is available for the treatment of prostate cancer in most developed countries,[80][38][81] including over 80 countries worldwide.[39][40] It is available in 50 mg, 80 mg (in Japan),[48] and 150 mg tablets for oral administration.[82][83] The drug is registered for use as a 150 mg/day monotherapy for the treatment of LAPC in at least 55 countries,[2] with the U.S. being a notable exception where it is registered only for use at a dosage of 50 mg/day in combination with castration.[84] No other formulations or routes of administration are available or used.[82] All formulations of bicalutamide are specifically indicated for the treatment of prostate cancer alone or in combination with surgical or medication castration.[4] Due to the low water solubility of bicalutamide, bicalutamide in oral bicalutamide tablets is micronized to ensure small and consistent particle sizes and optimize oral bioavailability.[85][2]
Bicalutamide is pregnancy category X, or "contraindicated in pregnancy", in the U.S.,[27] and pregnancy category D, the second most restricted rating, in Australia.[89] As such, it is contraindicated in women during pregnancy, and women who are sexually active and who can or may become pregnant are strongly recommended to take bicalutamide only in combination with adequate contraception.[90][91] It is unknown whether bicalutamide is excreted in breast milk, but many drugs are excreted in breast milk, and for this reason, bicalutamide treatment is similarly not recommended while breastfeeding.[3][27]
In individuals with severe, though not mild-to-moderate hepatic impairment, there is evidence that the elimination of bicalutamide is slowed, and hence, caution may be warranted in these patients as circulating levels of bicalutamide may be increased.[2][92] In severe hepatic impairment, the elimination half-life of the active (R)-enantiomer of bicalutamide is increased by about 1.75-fold (76% increase; elimination half-life of 5.9 and 10.4 days for normal and impaired patients, respectively).[13][93][94] The elimination half-life of bicalutamide is unchanged in renal impairment.[84]
^ abMay occur as often as 90% of those taking bicalutamide, but is mild-to-moderate in 90% of occurrences. Incidence greatly decreased in combination with castration.
^Usually transient, rarely severe. Resolves or improves with continued therapy or on discontinuation.
^ abReported in single cases, but not observed in any large, randomized trial. With regular liver monitoring and discontinuation as needed.
Bicalutamide has been associated with abnormal liver function tests such as elevated liver enzymes.[107][13] In the Early Prostate Cancer (EPC) clinical programme of bicalutamide for LPC and LAPC, the rate of abnormal liver function tests with bicalutamide monotherapy was 3.4% relative to 1.9% for placebo.[13][122] However, higher rates, up to 11%, have been seen in other studies.[18][27]Hepatic changes that have necessitated discontinuation of bicalutamide, such as marked increases in liver enzymes or hepatitis, have occurred in 0.3 to 1.5% of men in clinical trials, or approximately 1% overall.[27][13][33][122][123] Elevated liver enzymes with bicalutamide usually occur within the first 3 to 6 months of treatment.[107][27] Monitoring of liver function during treatment is recommended, particularly in the first few months.[13][102] In men with early prostate cancer, bicalutamide monotherapy has been found to increase non-prostate cancer mortality.[26][124][13] The reasons for the increase in mortality with bicalutamide in these men are unknown, but possible factors could include androgen deprivation or drug-related toxicity of bicalutamide.[125][126]
The side effect profile of bicalutamide in men and women differs from that of other antiandrogens and is considered favorable in comparison.[143][110][144][145] Relative to GnRH analogues and the steroidal antiandrogen (SAA) cyproterone acetate (CPA), bicalutamide monotherapy has a much lower incidence and severity of hot flashes and sexual dysfunction.[109][110][104][146] In addition, unlike GnRH analogues and CPA, bicalutamide monotherapy is not associated with decreased bone mineral density or osteoporosis.[104][110] Conversely, bicalutamide monotherapy is associated with much higher rates of breast tenderness, gynecomastia, and feminization in men than GnRH analogues and CPA.[104] However, gynecomastia with bicalutamide is rarely severe and discontinuation rates due to this side effect are fairly low.[104][110] These differences in side effects between bicalutamide monotherapy, GnRH analogues, and CPA are attributed to the fact that whereas GnRH analogues and CPA suppress estrogen production, bicalutamide monotherapy does not lower estrogen levels and in fact actually increases them.[104]
A single oral dose of bicalutamide in humans that results in symptoms of overdose or that is considered to be life-threatening has not been established.[27][163] Dosages of up to 600 mg/day have been well tolerated in clinical trials,[164] and it is notable that there is a saturation of absorption with bicalutamide such that circulating levels of its active (R)-enantiomer do not further increase above a dosage of 300 mg/day.[2][164] Overdose is considered unlikely to be life-threatening with bicalutamide or other first-generation NSAAs (i.e., flutamide and nilutamide).[165] A massive overdose of nilutamide (13 grams, or 43 times the normal maximum 300 mg/day clinical dosage) in a 79-year-old man was uneventful, producing no clinical signs, symptoms, or toxicity.[166] There is no specific antidote for bicalutamide or NSAA overdose, and treatment should be based on symptoms, if any are present.[27][163]
Interactions
Bicalutamide is almost exclusively metabolized by CYP3A4.[4] As such, its levels in the body may be altered by inhibitors and inducers of CYP3A4.[7] (For a list of CYP3A4 inhibitors and inducers, see here.) However, in spite of the fact bicalutamide is metabolized by CYP3A4, there is no evidence of clinically significant drug interactions when bicalutamide at a dosage of 150 mg/day or less is co-administered with drugs that inhibit or induce cytochrome P450enzyme activity.[13]
In-vitro studies suggest that bicalutamide may be able to inhibit CYP3A4 and, to a lesser extent, CYP2C9, CYP2C19, and CYP2D6.[2] Conversely, animal studies suggest that bicalutamide may induce cytochrome P450 enzymes.[2] In a clinical study, bicalutamide co-administered with the CYP3A4 substrate midazolam caused only a small and statistically non-significant increase in midazolam levels (+27%) presumably due to CYP3A4 inhibition.[2] However, this was well below increases in midazolam exposure with potent CYP3A4 inhibitors like ketoconazole (+1500%), itraconazole (+1000%), and erythromycin (+350%), and is considered to not be clinically important.[2] There is no indication of clinically significant enzyme inhibition or induction with bicalutamide at doses of 150mg/day or below.[2]
Because bicalutamide circulates at relatively high concentrations and is highly protein-bound, it has the potential to displace other highly protein-bound drugs like warfarin, phenytoin, theophylline, and aspirin from plasma binding proteins.[103][107] This could, in turn, result in increased free concentrations of such drugs and increased effects and/or side effects, potentially necessitating dosage adjustments.[103] Bicalutamide has specifically been found to displace coumarinanticoagulants like warfarin from their plasma binding proteins (namely albumin) in vitro, potentially resulting in an increased anticoagulant effect, and for this reason, close monitoring of prothrombin time and dosage adjustment as necessary is recommended when bicalutamide is used in combination with these drugs.[167][168][169] However, in spite of this, no conclusive evidence of an interaction between bicalutamide and other drugs was found in clinical trials of nearly 3,000 patients.[107]
The affinity of bicalutamide for the AR is relatively low as it is approximately 30 to 100 times lower than that of DHT, which is 2.5- to 10-fold as potent as an AR agonist as testosterone in bioassays and is the main endogenousligand of the receptor in the prostate gland.[180][172][2][181] However, typical clinical dosages of bicalutamide result in circulating levels of the drug that are thousands of times higher than those of testosterone and DHT, allowing it to powerfully prevent them from binding to and activating the receptor.[182][183][34][184][27][89][185][13][186] This is especially true in the case of surgical or medical castration, in which testosterone levels in the circulation are approximately 95% reduced and DHT levels in the prostate gland are about 50 to 60% reduced.[172][187] In women, levels of testosterone are substantially lower (20- to 40-fold) than in men,[188] so much smaller doses of bicalutamide (e.g., 25 mg/day in the hirsutism studies) are necessary.[17][52][189][33]
Blockade of the AR by bicalutamide in the pituitary gland and hypothalamus results in prevention of the negative feedback of androgens on the hypothalamic–pituitary–gonadal axis (HPG axis) in males and consequent disinhibition of pituitary luteinizing hormone (LH) secretion.[109] This, in turn, results in an increase in circulating LH levels and activation of the gonadal production of testosterone and by extension production of estradiol.[190] Levels of testosterone have been found to increase 1.5- to 2-fold (59–97% increase) and levels of estradiol about 1.5- to 2.5-fold (65–146% increase) in men treated with 150 mg/day bicalutamide monotherapy.[31][32][33] In addition to testosterone and estradiol, there are smaller increases in concentrations of DHT, sex hormone-binding globulin, and prolactin.[33] Estradiol levels with bicalutamide monotherapy are similar to those in the low-normal premenopausal female range while testosterone levels generally remain in the high end of the normal male range.[32][191][174] Testosterone concentrations do not typically exceed the normal male range due to negative feedback on the HPG axis by the increased concentrations of estradiol.[109] Bicalutamide influences the HPG axis and increases hormone levels only in men and not also in women.[192][193][194] This is due to the much lower levels of androgens in women and their lack of basal suppression of the HPG axis in this sex.[192][193][194] As evidenced by its effectiveness in the treatment of prostate cancer and other androgen-dependent conditions, the antiandrogenic actions of bicalutamide considerably exceed any impact of the increased levels of testosterone it results in.[84] However, the elevated levels of estradiol remain unopposed by bicalutamide and are responsible for the gynecomastia and feminizing side effects it causes in men.[195] Although bicalutamide monotherapy increases gonadotropin and sex hormone levels in men, this will not occur if bicalutamide is combined with an antigonadotropin such as a GnRH analogue, estrogen, or progestogen, as these medications maintain negative feedback on the HPG axis.[50][196][197]
NSAA monotherapy, including with bicalutamide, shows a number of tolerability differences from methods of androgen deprivation therapy that incorporate surgical or medical castration. For example, the rates of hot flashes, depression, fatigue, and sexual dysfunction are all much higher with GnRH analogues than with NSAA monotherapy. It is thought that this is because GnRH analogues suppress estrogen production in addition to androgen production, resulting in estrogen deficiency.[198][199][200] In contrast, NSAA monotherapy does not decrease estrogen levels and in fact increases them, resulting in an excess of estrogens that compensates for androgen deficiency and allows for a preservation of mood, energy, and sexual function.[198][199][200]Neurosteroids that are produced from testosterone like 3α-androstanediol and 3β-androstanediol, which are ERβTooltip estrogen receptor beta agonists and the former a potent GABAA receptorpositive allosteric modulator, may also be involved.[201][202][203][204][205][206][207] In the specific case of sexual dysfunction, an additional possibility for the difference is that without concomitant suppression of androgen production, blockade of the AR by the bicalutamide in the brain is incomplete and insufficient to markedly influence sexual function.[citation needed]
Under normal circumstances, bicalutamide has no capacity to activate the AR.[208][209] However, in prostate cancer, mutations and overexpression of the AR can accumulate in prostate gland cells which can convert bicalutamide from an antagonist of the AR into an agonist.[208][210] This can result in paradoxical stimulation of prostate cancer growth with bicalutamide and is responsible for the phenomenon of the antiandrogen withdrawal syndrome, where antiandrogen discontinuation paradoxically slows the rate of prostate cancer growth.[208][210]
In transgender women, breast development is a desired effect of antiandrogen or estrogen treatment.[63][211] Breast development and gynecomastia induced by bicalutamide is thought to be mediated by increased activation of the ER secondary to blockade of the AR (resulting in disinhibition of the ER in breast tissue) and increased levels of estradiol.[20][212][213] In addition to fat deposition, connective tissue growth, and ductal development, bicalutamide has been found to produce moderate lobuloalveolar development of the breasts.[214][215][216] However, full lobuloalveolar maturation necessary for lactation and breastfeeding will not occur without progestogen treatment.[214][215][216]
Bicalutamide monotherapy seems to have minimal effect on testicularspermatogenesis, testicular ultrastructure, and certain aspects of male fertility.[217][90][218] This seems to be because testosterone levels in the testes (where ~95% of testosterone in males is produced) are extremely high (up to 200-fold higher than circulating levels) and only a small fraction (less than 10%) of the normal levels of testosterone in the testes are actually necessary to maintain spermatogenesis.[219][220][221] As a result, bicalutamide appears to not be able to compete with testosterone in this sole part of the body to an extent sufficient to considerably interfere with androgen signaling and function.[219][220][221] However, while bicalutamide does not seem to be able to adversely influence testicular spermatogenesis, it may interfere with AR-dependent sperm maturation and transport outside of the testes in the epididymides and vas deferens where androgen levels are far lower, and hence may still be able to impair male fertility.[222] In addition, the combination of bicalutamide with other medications, such as estrogens, progestogens, and GnRH analogues, can compromise spermatogenesis due to their own adverse effects on male fertility.[223][224][225][226][227][228] These medications are able to strongly suppress gonadal androgen production, which can severely impair or abolish testicular spermatogenesis, and estrogens also appear to have direct and potentially long-lasting cytotoxic effects in the testes at sufficiently high concentrations.[223][224][225][226][227][228]
Other activities
Bicalutamide has been found to act as an inhibitor or inducer of certain cytochrome P450enzymes including CYP3A4, CYP2C9, CYP2C19, and CYP2D6 in preclinical research, but no evidence of this has been found in humans treated with up to 150 mg/day.[2] It has also been identified in vitro as a strong inhibitor of CYP27A1 (cholesterol 27-hydroxylase) and as an inhibitor of CYP46A1 (cholesterol 24-hydroxylase), but this has yet to be assessed or confirmed in vivo or in humans and the clinical significance remains unknown.[229][230] Bicalutamide has been found to be a P-glycoprotein (ABCB1) inhibitor.[231][232][233] Like other first-generation NSAAs and enzalutamide, it has been found to act as a weak non-competitive inhibitor of GABAA receptor-mediated currentsin vitro (IC50 = 5.2 μM).[234][235] However, unlike enzalutamide, bicalutamide has not been found to be associated with seizures or other related adverse central effects, so the clinical relevance of this finding is uncertain.[234][235]
Though its absolute bioavailability in humans is unknown, bicalutamide is known to be extensively and well-absorbed.[2][3] Its absorption is not affected by food.[3][167] The absorption of bicalutamide is linear at doses up to 150 mg/day and is saturable at doses above this, with no further increases in steady-state levels of bicalutamide occurring at doses above 300 mg/day.[2][13][236][164] Whereas absorption of (R)-bicalutamide is slow, with levels peaking at 31 to 39 hours after a dose, (S)-bicalutamide is much more rapidly absorbed.[13][27][2] Steady-state concentrations of the drug are reached after 4 to 12 weeks of treatment independently of dosage, with a 10- to 20-fold progressive accumulation in levels of (R)-bicalutamide.[13][237][238][185] The long time to steady-state levels is the result of bicalutamide's very long elimination half-life.[185] There is wide interindividual variability in (R)-bicalutamide levels (up to 16-fold) with bicalutamide regardless of dosage.[2]
The tissue distribution of bicalutamide is not well-characterized.[239] The amount of bicalutamide in semen that could potentially be transferred to a female partner during sexual intercourse is low and is not thought to be important.[89] Based on animal studies with rats and dogs it was thought that bicalutamide could not cross the blood–brain barrier and hence could not enter the brain.[240][34][241][242] As such, it was initially thought to be a peripherally selective antiandrogen.[240][34] However, subsequent clinical studies found that this was not also the case for humans, indicating species differences; bicalutamide crosses into the human brain and, in accordance, produces effects and side effects consistent with central antiandrogenic action.[2][109][243][244][245] In any case, there is indication that bicalutamide might have at least some peripheral selectivity in humans.[246] Bicalutamide is highly plasma protein bound (96.1% for racemic bicalutamide, 99.6% for (R)-bicalutamide) and is bound mainly to albumin, with negligible binding to SHBG and corticosteroid-binding globulin.[4][2][239][176]
Bicalutamide is metabolized in the liver.[4][167] (R)-Bicalutamide is metabolized slowly and almost exclusively via hydroxylation by CYP3A4 into (R)-hydroxybicalutamide.[167][2][4][247] This metabolite is then glucuronidated by UGT1A9.[167][2][9][6] In contrast to (R)-bicalutamide, (S)-bicalutamide is metabolized rapidly and mainly by glucuronidation (without hydroxylation).[167] None of the metabolites of bicalutamide are known to be active and levels of the metabolites are low in plasma, where unchanged biclautamide predominates.[4][5][2] Due to the stereoselective metabolism of bicalutamide, (R)-bicalutamide has a far longer terminal half-life than (S)-bicalutamide and its levels are about 10- to 20-fold higher in comparison following a single dose and 100-fold higher at steady-state.[13][247][248] (R)-Bicalutamide has a relatively long elimination half-life of 5.8 days with a single dose and 7 to 10 days following repeated administration.[8]
Bicalutamide is eliminated in similar proportions in feces (43%) and urine (34%), while its metabolites are eliminated roughly equally in urine and bile.[4][167][249][250] The drug is excreted to a substantial extent in unmetabolized form, and both bicalutamide and its metabolites are eliminated mainly as glucuronideconjugates.[173] The glucuronide conjugates of bicalutamide and its metabolites are eliminated from the circulation rapidly, unlike unconjugated bicalutamide.[2][167][251]
First-generation NSAAs including bicalutamide, flutamide, and nilutamide are all synthetic, nonsteroidal anilide derivatives and structural analogues of each other.[255] Bicalutamide is a diarylpropionamide while flutamide is a monoarylpropionamide and nilutamide is a hydantoin.[255] Bicalutamide and flutamide, though not nilutamide, can also be classified as toluidides.[247] All three of the compounds share a common 3-trifluoromethylaniline moiety.[256] Bicalutamide is a modification of flutamide in which a 4-fluorophenylsulfonyl moiety has been added and the nitro group on the original phenyl ring has been replaced with a cyano group.[257]Topilutamide, also known as fluridil, is another NSAA that is closely related structurally to the first-generation NSAAs, but, in contrast to them, is not used in the treatment of prostate cancer and is instead used exclusively as a topical antiandrogen in the treatment of pattern hair loss.[258][259][260]
The second-generation NSAAs enzalutamide and apalutamide were derived from and are analogues of the first-generation NSAAs,[167][261] while another second-generation NSAA, darolutamide, is said to be structurally distinct and chemically unrelated to the other NSAAs.[262] Enzalutamide is a modification of bicalutamide in which the inter-ring linking chain has been altered and cyclized into a 5,5-dimethyl-4-oxo-2-thioxoimidazolidine moiety. In apalutamide, the 5,5-dimethyl groups of the imidazolidine ring of enzalutamide are cyclized to form an accessory cyclobutane ring and one of its phenyl rings is replaced with a pyridine ring.
The first nonsteroidal androgens, the arylpropionamides, were discovered via structural modification of bicalutamide.[263] Unlike bicalutamide (which is purely antiandrogenic), these compounds show tissue-selective androgenic effects and were classified as selective androgen receptor modulators (SARMs).[263] Lead SARMs of this series included acetothiolutamide, enobosarm (ostarine; S-22), and andarine (acetamidoxolutamide or androxolutamide; S-4).[255][263][264] They are very close to bicalutamide structurally, with the key differences being that the linker sulfone of bicalutamide has been replaced with an ether or thioether group to confer agonism of the AR and the 4-fluoro atom of the pertinent phenyl ring has been substituted with an acetamido or cyano group to eliminate reactivity at the position.[265]
A few radiolabeled derivatives of bicalutamide have been developed for potential use as radiotracers in medical imaging.[266][267] They include [18F]bicalutamide, 4-[76Br]bromobicalutamide, and [76Br]bromo-thiobicalutamide.[266][267] The latter two were found to have substantially increased affinity for the AR relative to that of bicautamide.[266] However, none of these agents have been evaluated in humans.[266][267]
5N-Bicalutamide, or 5-azabicalutamide, is a minor structural modification of bicalutamide which acts as a reversible covalent antagonist of the AR and has approximately 150-fold higher affinity for the AR and about 20-fold greater functional inhibition of the AR relative to bicalutamide.[268][269] It is among the most potent AR antagonists to have been developed and is being researched for potential use in the treatment of antiandrogen-resistant prostate cancer.[268]
Synthesis
A number of chemical syntheses of bicalutamide have been published in the literature.[252][270][271][272][273] The procedure of the first published synthesis of bicalutamide can be seen below.[270]
Bicalutamide as well as all of the other currently marketed NSAAs were derived from structural modification of flutamide, which itself was originally synthesized as a bacteriostatic agent in 1967 at Schering Plough Corporation and was subsequently and serendipitously found to possess antiandrogenic activity.[274][275][276] Bicalutamide was discovered by Tucker and colleagues at Imperial Chemical Industries (ICI) in the 1980s and was selected for development from a group of over 2,000 synthesized compounds.[277][176][278][252] It was first patented in 1982[279] and was first reported in the scientific literature in June 1987.[280]
Bicalutamide was first studied in a phase Iclinical trial in 1987[107] and the results of the first phase II clinical trial in prostate cancer were published in 1990.[281] The pharmaceutical division of ICI was split out into an independent company called Zeneca in 1993, and in April and May 1995, Zeneca (now AstraZeneca, after merging with Astra AB in 1999) began pre-approval marketing of bicalutamide for the treatment of prostate cancer in the U.S..[282] It was first launched in the U.K.Tooltip United Kingdom in May 1995,[283] and was subsequently approved by the U.S. FDA on 4 October 1995, for the treatment of prostate cancer at a dosage of 50 mg/day in combination with a GnRH analogue.[284][285]
Following its introduction for use in combination with a GnRH analogue, bicalutamide was developed as a monotherapy at a dosage of 150 mg/day for the treatment of prostate cancer, and was approved for this indication in Europe, Canada, and a number of other countries in the late 1990s and early 2000s.[13][172][286][287] This application of bicalutamide was also under review by the FDA in the U.S. in 2002,[288] but ultimately was not approved in this country.[84] In Japan, bicalutamide is licensed at a dosage of 80 mg/day alone or in combination with a GnRH analogue for prostate cancer.[48] The unique 80 mg dosage of bicalutamide used in Japan was selected for development in this country on the basis of observed pharmacokinetic differences with bicalutamide in Japanese men.[49]
Subsequent to negative findings of bicalutamide monotherapy for LPC in the EPC clinical programme, approval of bicalutamide for use specifically in the treatment of LPC was withdrawn in a number of countries[14] including the U.K. (in October or November 2003)[15] and several other European countries and Canada (in August 2003).[13][289][290] In addition, the U.S. and Canada explicitly recommended against the use of 150 mg/day bicalutamide for this indication.[16] The drug is effective for, remains approved for, and continues to be used in the treatment of LAPC and mPC, on the other hand.[13]
The patent protection of bicalutamide expired in the U.S. in March 2009 and the drug has subsequently been available as a generic,[291] at greatly reduced cost.[292]
Bicalutamide was the fourth antiandrogen (and the third NSAA) to be introduced for the treatment of prostate cancer, following the SAA CPA in 1973[293] and the NSAAs flutamide in 1983 (1989 in the U.S.)[252][294] and nilutamide in 1989 (1996 in the U.S.).[256][295][296] It has been followed by abiraterone acetate in 2011, enzalutamide in 2012, apalutamide in 2018, and darolutamide in 2019, and may also be followed by in-development drugs such as proxalutamide and seviteronel.[297]
Society and culture
Generic names
Bicalutamide is the generic name of the drug in English and French and its INNTooltip INN, USANTooltip United States Adopted Name, USPTooltip United States Pharmacopeia,[298]BANTooltip British Approved Name, DCFTooltip Dénomination Commune Française, AANTooltip Australian Approved Name,[89] and JANTooltip Japanese Accepted Name.[38][299][80][300] It is also referred to as bicalutamidum in Latin, bicalutamida in Spanish and Portuguese, bicalutamid in German, and bikalutamid in Russian and other Slavic languages.[38][80] The "bica-" prefix corresponds to the fact that bicalutamide is a bicyclic compound, while the "-lutamide" suffix is the standard suffix for NSAAs.[301][302] Bicalutamide is also known by its former developmental code name ICI-176,334.[299][80][38]
Brand names
Bicalutamide is marketed by AstraZeneca in oral tablet form under the brand names Casodex, Cosudex, Calutide, Calumid, and Kalumid in many countries.[38][80][303][304] It is also marketed under the brand names Bicadex, Bical, Bicalox, Bicamide, Bicatlon, Bicusan, Binabic, Bypro, Calutol, and Ormandyl among others in various countries.[38] The drug is sold under a large number of generic trade names such as Apo-Bicalutamide, Bicalutamide Accord, Bicalutamide Actavis, Bicalutamide Bluefish, Bicalutamide Kabi, Bicalutamide Sandoz, and Bicalutamide Teva as well.[38] A combination formulation of bicalutamide and goserelin is marketed by AstraZeneca in Australia and New Zealand under the brand name ZolaCos-CP.[81][86][87][88]
Cost and generics
Bicalutamide is off-patent and available as a generic.[291] Unlike bicalutamide, the newer NSAA enzalutamide is still on-patent, and for this reason, is considerably more expensive in comparison.[305]
The patent protection of all three of the first-generation NSAAs has expired and flutamide and bicalutamide are both available as low-cost generics.[306][307] Nilutamide, on the other hand, has always been a poor third competitor to flutamide and bicalutamide and, in relation to this fact, has not been developed as a generic and is only available as brand name Nilandron, at least in the U.S.[306][307]
Bicalutamide is considerably less costly than GnRH analogues, which, in spite of some having been off-patent many years, have been reported (in 2013) to typically cost US$10,000–$15,000 per year (or about US$1,000 per month) of treatment.[308][309]
Sales and usage
Sales of bicalutamide (as Casodex) worldwide peaked at US$1.3 billion in 2007,[310] and it has been described as a "billion-dollar-a-year" drug prior to losing its patent protection starting in 2007.[43][311][258] In 2014, despite the introduction of abiraterone acetate in 2011 and enzalutamide in 2012, bicalutamide was still the most commonly prescribed drug in the treatment of metastatic castration-resistant prostate cancer (mCRPC).[43] Moreover, in spite of being off-patent, bicalutamide was said to still generate a few hundred million dollars in sales per year for AstraZeneca.[43] Total worldwide sales of brand name Casodex were approximately US$13.4 billion as of the end of 2018.[312][313][40][314][315][310][316][317][318][319][320][excessive citations]
Worldwide sales (millions, USD) of Casodex, 1995–2018
Between January 2007 and December 2009 (a period of three years), 1,232,143 prescriptions of bicalutamide were dispensed in the U.S., or about 400,000 prescriptions per year.[44] During that time, bicalutamide accounted for about 87.2% of the NSAA market, while flutamide accounted for 10.5% of it and nilutamide for 2.3% of it.[44] Approximately 96% of bicalutamide prescriptions were written for diagnosis codes that clearly indicated neoplasm.[44] About 1,200, or 0.1% of bicalutamide prescriptions were dispensed to pediatric patients (age 0–16).[44]
Bicalutamide has been studied in the treatment of benign prostatic hyperplasia (BPH) in a 24-week trial of 15 patients at a dosage of 50 mg/day.[339][340] Prostate volume decreased by 26% in patients taking bicalutamide and urinary irritative symptom scores significantly decreased.[339][340] Conversely, peak urine flow rates and urine pressure flow examinations were not significantly different between bicalutamide and placebo.[339][340] The decrease in prostate volume achieved with bicalutamide was comparable to that observed with the 5α-reductase inhibitor finasteride, which is approved for the treatment of BPH.[341][342] Breast tenderness (93%), gynecomastia (54%), and sexual dysfunction (60%) were all reported as side effects of bicalutamide at the dosage used in the study, although no treatment discontinuations due to adverse effects occurred and sexual functioning was maintained in 75% of patients.[340][107]
A phase III clinical trial of bicalutamide in combination with an ethinylestradiol-containing combined oral contraceptive for the treatment of severe hirsutism in women with PCOS was completed in Italy in 2017 under supervision of the Italian Agency for Drugs (AIFA).[57]
Antiandrogens have been suggested for treating COVID-19 in men and as of May 2020 high-dose bicalutamide is in a phase II clinical trial for this purpose.[343][344]
Veterinary use
Bicalutamide may be used to treat hyperandrogenism and associated benign prostatic hyperplasia secondary to hyperadrenocorticism (caused by excessive adrenal androgens) in male ferrets.[345][346][347] However, it has not been formally assessed in controlled studies for this purpose.[347][348]
^ abDole EJ, Holdsworth MT (1997). "Nilutamide: an antiandrogen for the treatment of prostate cancer". The Annals of Pharmacotherapy. 31 (1): 65–75. doi:10.1177/106002809703100112. PMID8997470. S2CID20347526. page 67: Currently, information is not available regarding the activity of the major urinary metabolites of bicalutamide, bicalutamide glucuronide, and hydroxybicalutamide glucuronide.
^ abSchellhammer PF (September 2002). "An evaluation of bicalutamide in the treatment of prostate cancer". Expert Opinion on Pharmacotherapy. 3 (9): 1313–28. doi:10.1517/14656566.3.9.1313. PMID12186624. S2CID32216411. The clearance of bicalutamide occurs pre- dominantly by hepatic metabolism and glucuronidation, with excretion of the resulting inactive metabolites in the urine and faces.
^ abcdefghij"Bicalutamide". The American Society of Health-System Pharmacists. Archived from the original on 29 December 2016. Retrieved 8 December 2016.
^ abNargund VH, Raghavan D, Sandler HM (17 January 2015). Urological Oncology. Springer. pp. 823–. ISBN978-0-85729-482-1. On the other hand, the 150 mg dose of bicalutamide has been associated with some safety concerns, such as a higher death rate when added to active surveillance in the early prostate cancer trialists group study [29], which has led the United States and Canada to recommend against prescribing the 150 mg dose [30].
^ abElliott S, Latini DM, Walker LM, Wassersug R, Robinson JW (2010). "Androgen deprivation therapy for prostate cancer: recommendations to improve patient and partner quality of life". The Journal of Sexual Medicine. 7 (9): 2996–3010. doi:10.1111/j.1743-6109.2010.01902.x. PMID20626600.
^ abHammerer P, Manka L (2019). "Androgen Deprivation Therapy for Advanced Prostate Cancer". Urologic Oncology. Springer International Publishing. pp. 255–276. doi:10.1007/978-3-319-42623-5_77. ISBN978-3-319-42622-8. Bicalutamide is the most widely used antiandrogen in the treatment of prostate cancer. [...] Common side effects [of bicalutamide] include breast enlargement, breast tenderness, hot flashes, and constipation as well as feminization and changes in mood and liver as well as lung toxicity; monitoring of liver enzymes is recommended during treatment (Schellhammer and Davis 2004).
^ abJia AY, Spratt DE (June 2022). "Bicalutamide Monotherapy With Radiation Therapy for Localized Prostate Cancer: A Non-Evidence-Based Alternative". Int J Radiat Oncol Biol Phys. 113 (2): 316–319. doi:10.1016/j.ijrobp.2022.01.037. PMID35569476. S2CID248765294. Four other randomized trials using BICmono have also raised concerns about either lack of efficacy or even harm from this treatment approach compared with placebo or no hormone therapy. SPCG-6 randomized 1218 patients to either 150 mg of BICmono daily or placebo. In the subset of patients with LPCa managed with observation, survival was significantly worse with BIC than placebo (hazard ratio [HR], 1.47; 95% confidence interval, 1.06-2.03).10 Two other randomized trials were part of the early prostate cancer program,11 which conducted 3 randomized trials that were pooled together to determine the benefit of BICmono (SPCG-6 was one of the 3 trials). Overall, in the combined 8113 patient pooled cohort, after a median follow-up of 7 years, there was no improvement even in progression-free survival from the use of adjuvant BIC in LPCa, and there was a trend for worse overall survival (HR, 1.16; 95% confidence interval, 0.99-1.37; P = .07). [...] Although not in LPCa, NRG/RTOG 9601 demonstrated findings consistent with the prior trials.12 This trial randomized men to postprostatectomy salvage radiation therapy plus placebo versus 150 mg of BICmono daily for 2 years. After a median follow-up of 13 years, the trial showed that there were significantly more grade 3 to 5 cardiac events in the BICmono arm. In patients with less aggressive disease with lower PSAs (prostate-specific antigens; more analogous to LPCa), other-cause mortality was significantly higher in the BICmono arm. In patients with high PSAs >1.5 ng/mL (which with modern molecular positron emission tomography imaging would be expected to have high rates of regional and distant metastatic disease), a survival benefit from the addition of BIC was observed. This is consistent with results from the early prostate cancer studies that showed that only patients with more advanced disease derived benefit from BICmono.10 Thus, all the randomized evidence from 5 trials (Table 1) demonstrates that, in LPCa, BICmono had no clinically significant oncologic activity over placebo/no treatment, and consistent trends with long-term use resulted in worse survival.
^ abLee K, Oda Y, Sakaguchi M, Yamamoto A, Nishigori C (May 2016). "Drug-induced photosensitivity to bicalutamide – case report and review of the literature". Photodermatology, Photoimmunology & Photomedicine. 32 (3): 161–4. doi:10.1111/phpp.12230. PMID26663090. S2CID2761388.
^ abcdeFurr BJ, Tucker H (January 1996). "The preclinical development of bicalutamide: pharmacodynamics and mechanism of action". Urology. 47 (1A Suppl): 13–25, discussion 29–32. doi:10.1016/S0090-4295(96)80003-3. PMID8560673.
^World Health Organization (2019). World Health Organization model list of essential medicines: 21st list 2019. Geneva: World Health Organization. hdl:10665/325771. WHO/MVP/EMP/IAU/2019.06. License: CC BY-NC-SA 3.0 IGO.
^Hamilton R (2015). Tarascon Pocket Pharmacopoeia 2015 Deluxe Lab-Coat Edition. Jones & Bartlett Learning. p. 381. ISBN9781284057560.
^ abAkaza H (1999). "[A new anti-androgen, bicalutamide (Casodex), for the treatment of prostate cancer—basic clinical aspects]". Gan to Kagaku Ryoho. Cancer & Chemotherapy (in Japanese). 26 (8): 1201–7. PMID10431591.
^ abcdCampbell T (22 January 2014). "Slowing Sales for Johnson & Johnson's Zytiga May Be Good News for Medivation". The Motley Fool. Archived from the original on 26 August 2016. Retrieved 20 July 2016. [...] the most commonly prescribed treatment for metastatic castration resistant prostate cancer: bicalutamide. That was sold as AstraZeneca's billion-dollar-a-year drug Casodex before losing patent protection in 2008. AstraZeneca still generates a few hundred million dollars in sales from Casodex, [...]
^Klotz L, Schellhammer P (March 2005). "Combined androgen blockade: the case for bicalutamide". Clinical Prostate Cancer. 3 (4): 215–9. doi:10.3816/cgc.2005.n.002. PMID15882477.
^Schellhammer PF, Sharifi R, Block NL, Soloway MS, Venner PM, Patterson AL, Sarosdy MF, Vogelzang NJ, Schellenger JJ, Kolvenbag GJ (September 1997). "Clinical benefits of bicalutamide compared with flutamide in combined androgen blockade for patients with advanced prostatic carcinoma: final report of a double-blind, randomized, multicenter trial. Casodex Combination Study Group". Urology. 50 (3): 330–6. doi:10.1016/S0090-4295(97)00279-3. PMID9301693.
^ abcSuzuki H, Kamiya N, Imamoto T, Kawamura K, Yano M, Takano M, Utsumi T, Naya Y, Ichikawa T (October 2008). "Current topics and perspectives relating to hormone therapy for prostate cancer". International Journal of Clinical Oncology. 13 (5): 401–10. doi:10.1007/s10147-008-0830-y. PMID18946750. S2CID32859879.
^ abMelmed S (1 January 2016). Williams Textbook of Endocrinology. Elsevier Health Sciences. pp. 752–. ISBN978-0-323-29738-7. GnRH analogues, both agonists and antagonists, severely suppress endogenous gonadotropin and testosterone production [...] Administration of GnRH agonists (e.g., leuprolide, goserelin) produces an initial stimulation of gonadotropin and testosterone secretion (known as a "flare"), which is followed in 1 to 2 weeks by GnRH receptor downregulation and marked suppression of gonadotropins and testosterone to castration levels. [...] To prevent the potential complications associated with the testosterone flare, AR antagonists (e.g., bicalutamide) are usually coadministered with a GnRH agonist for men with metastatic prostate cancer.399
^Gooren LJ (March 2011). "Clinical practice. Care of transsexual persons". The New England Journal of Medicine. 364 (13): 1251–1257. doi:10.1056/nejmcp1008161. PMID21449788.
^ abWierckx K, Gooren L, T'Sjoen G (May 2014). "Clinical review: Breast development in trans women receiving cross-sex hormones". The Journal of Sexual Medicine. 11 (5): 1240–1247. doi:10.1111/jsm.12487. PMID24618412.
^Haddad NG, Eugster EA (June 2019). "Peripheral precocious puberty including congenital adrenal hyperplasia: causes, consequences, management and outcomes". Best Practice & Research. Clinical Endocrinology & Metabolism. 33 (3): 101273. doi:10.1016/j.beem.2019.04.007. hdl:1805/19111. PMID31027974. S2CID135410503.
^Haddad NG, Eugster EA (2012). "Peripheral Precocious Puberty: Interventions to Improve Growth". Handbook of Growth and Growth Monitoring in Health and Disease. Springer. pp. 1199–1212. doi:10.1007/978-1-4419-1795-9_71. ISBN978-1-4419-1794-2.
^Reiter EO, Mauras N, McCormick K, Kulshreshtha B, Amrhein J, De Luca F, et al. (October 2010). "Bicalutamide plus anastrozole for the treatment of gonadotropin-independent precocious puberty in boys with testotoxicosis: a phase II, open-label pilot study (BATT)". Journal of Pediatric Endocrinology & Metabolism. 23 (10): 999–1009. doi:10.1515/jpem.2010.161. PMID21158211. S2CID110630.
^Broderick GA, Kadioglu A, Bivalacqua TJ, Ghanem H, Nehra A, Shamloul R (January 2010). "Priapism: pathogenesis, epidemiology, and management". The Journal of Sexual Medicine. 7 (1 Pt 2): 476–500. doi:10.1111/j.1743-6109.2009.01625.x. PMID20092449.
^Giltay EJ, Gooren LJ (2009). "Potential side effects of androgen deprivation treatment in sex offenders". The Journal of the American Academy of Psychiatry and the Law. 37 (1): 53–8. PMID19297634.
^Khan O, Mashru A (2016). "The efficacy, safety and ethics of the use of testosterone-suppressing agents in the management of sex offending". Current Opinion in Endocrinology, Diabetes and Obesity. 23 (3): 271–8. doi:10.1097/MED.0000000000000257. PMID27032060. S2CID43286710.
^Rousseau L, Couture M, Dupont A, Labrie F, Couture N (1990). "Effect of combined androgen blockade with an LHRH agonist and flutamide in one severe case of male exhibitionism". The Canadian Journal of Psychiatry. 35 (4): 338–41. doi:10.1177/070674379003500412. PMID2189544. S2CID28970865.
^ abcdeChabner BA, Longo DL (8 November 2010). Cancer Chemotherapy and Biotherapy: Principles and Practice. Lippincott Williams & Wilkins. pp. 679–680. ISBN978-1-60547-431-1. Archived from the original on 10 January 2023. Retrieved 27 September 2016. From a structural standpoint, antiandrogens are classified as steroidal, including cyproterone [acetate] (Androcur) and megestrol [acetate], or nonsteroidal, including flutamide (Eulexin, others), bicalutamide (Casodex), and nilutamide (Nilandron). The steroidal antiandrogens are rarely used.
^Kolvenbag GJ, Furr BJ, Blackledge GR (December 1998). "Receptor affinity and potency of non-steroidal antiandrogens: translation of preclinical findings into clinical activity". Prostate Cancer Prostatic Dis. 1 (6): 307–314. doi:10.1038/sj.pcan.4500262. PMID12496872. S2CID33497597. In addition, since bicalutamide has a low solubility, authentic Casodex® is micronised to ensure a small and consistent particle size to optimise bioavailability.
^"Bicalutamide"(PDF). Richmond Hill, Ontario: Nu-Pharm Inc. October 2009.
^Bennett CL, Raisch DW, Sartor O (October 2002). "Pneumonitis associated with nonsteroidal antiandrogens: presumptive evidence of a class effect". Annals of Internal Medicine. 137 (7): 625. doi:10.7326/0003-4819-137-7-200210010-00029. PMID12353966. An estimated 0.77% of the 6,480 nilutamide-treated patients, 0.04% of the 41,700 flutamide-treated patients, and 0.01% of the 86,800 bicalutamide-treated patients developed pneumonitis during the study period.
^Molina Mancero G, Picón X, Di Tullio F, Ernst G, Dezanzo P, Salvado A, Chertcoff JF (October 2016). "Neumonía intersticial inducida por bloqueo androgénico máximo como tratamiento de cáncer de próstata avanzado" [Fatal interstitial lung disease associated with maximum androgen blockade. Report of one case]. Revista médica de Chile (in Spanish). 144 (10): 1356–1359. doi:10.4067/S0034-98872016001000017. PMID28074993.
^Lee K, Oda Y, Sakaguchi M, Yamamoto A, Nishigori C (May 2016). "Drug-induced photosensitivity to bicalutamide - case report and review of the literature". Photodermatology, Photoimmunology & Photomedicine. 32 (3): 161–164. doi:10.1111/phpp.12230. PMID26663090. S2CID2761388.
^Gretarsdottir HM, Bjornsdottir E, Bjornsson ES (2018). "Bicalutamide-Associated Acute Liver Injury and Migratory Arthralgia: A Rare but Clinically Important Adverse Effect". Case Reports in Gastroenterology. 12 (2): 266–270. doi:10.1159/000485175. ISSN1662-0631. S2CID81661015.
^ abcdWirth MP, Hakenberg OW, Froehner M (February 2007). "Antiandrogens in the treatment of prostate cancer". European Urology. 51 (2): 306–13, discussion 314. doi:10.1016/j.eururo.2006.08.043. PMID17007995.
^Higano CS (2012). "Sexuality and intimacy after definitive treatment and subsequent androgen deprivation therapy for prostate cancer". Journal of Clinical Oncology. 30 (30): 3720–5. doi:10.1200/JCO.2012.41.8509. PMID23008326.
^ abcdefghKolvenbag GJ, Blackledge GR (January 1996). "Worldwide activity and safety of bicalutamide: a summary review". Urology. 47 (1A Suppl): 70–9, discussion 80–4. doi:10.1016/s0090-4295(96)80012-4. PMID8560681. Bicalutamide is a new antiandrogen that offers the convenience of once-daily administration, demonstrated activity in prostate cancer, and an excellent safety profile. Because it is effective and offers better tolerability than flutamide, bicalutamide represents a valid first choice for antiandrogen therapy in combination with castration for the treatment of patients with advanced prostate cancer.
^Kathryn Korkidakis A, Reid RL (2017). "Testosterone in Women: Measurement and Therapeutic Use". Journal of Obstetrics and Gynaecology Canada. 39 (3): 124–130. doi:10.1016/j.jogc.2017.01.006. PMID28343552.
^Davis SR, Wahlin-Jacobsen S (2015). "Testosterone in women--the clinical significance". The Lancet Diabetes & Endocrinology. 3 (12): 980–92. doi:10.1016/S2213-8587(15)00284-3. PMID26358173.
^Luque-Ramírez M, Ortiz-Flores AE, Nattero-Chávez L, Escobar-Morreale HF (December 2020). "A safety evaluation of current medications for adult women with the polycystic ovarian syndrome not pursuing pregnancy". Expert Opin Drug Saf. 19 (12): 1559–1576. doi:10.1080/14740338.2020.1839409. PMID33070640. S2CID224784192.
^Fourcade RO, McLeod D (March 2004). "Tolerability of Antiandrogens in the Treatment of Prostate Cancer". UroOncology. 4 (1): 5–13. doi:10.1080/1561095042000191655. ISSN1561-0950. Based on the available evidence, bicalutamide appears to have a better profile of non-pharmacological side effects than either flutamide or nilutamide; no specific nonpharmacological complications have yet been linked to this agent, while the incidence of the side effects such as diarrhoea and abnormal liver function appears to be lower than for the other two non-steroidal compounds. Furthermore, the recent data from the EPC programme suggest that the non-pharmacological side-effect profile of bicalutamide is not dissimilar to that of placebo (Table m [3].
^Lunglmayr G (August 1995). "Efficacy and tolerability of Casodex in patients with advanced prostate cancer. International Casodex Study Group". Anti-Cancer Drugs. 6 (4): 508–13. doi:10.1097/00001813-199508000-00003. PMID7579554.
^Tyrrell CJ, Iversen P, Tammela T, Anderson J, Björk T, Kaisary AV, Morris T (September 2006). "Tolerability, efficacy and pharmacokinetics of bicalutamide 300 mg, 450 mg or 600 mg as monotherapy for patients with locally advanced or metastatic prostate cancer, compared with castration". BJU International. 98 (3): 563–72. doi:10.1111/j.1464-410X.2006.06275.x. PMID16771791. S2CID41672303.
^ abSee WA, Wirth MP, McLeod DG, Iversen P, Klimberg I, Gleason D, et al. (August 2002). "Bicalutamide as immediate therapy either alone or as adjuvant to standard care of patients with localized or locally advanced prostate cancer: first analysis of the early prostate cancer program". The Journal of Urology. 168 (2): 429–35. doi:10.1016/S0022-5347(05)64652-6. PMID12131282.
^Schellhammer P, Sharifi R, Block N, Soloway M, Venner P, Patterson AL, Sarosdy M, Vogelzang N, Jones J, Kolvenbag G (January 1996). "Maximal androgen blockade for patients with metastatic prostate cancer: outcome of a controlled trial of bicalutamide versus flutamide, each in combination with luteinizing hormone-releasing hormone analogue therapy. Casodex Combination Study Group". Urology. 47 (1A Suppl): 54–60, discussion 80–4. doi:10.1016/s0090-4295(96)80010-0. PMID8560679.
^Iversen P, Johansson JE, Lodding P, Lukkarinen O, Lundmo P, Klarskov P, Tammela TL, Tasdemir I, Morris T, Carroll K (November 2004). "Bicalutamide (150 mg) versus placebo as immediate therapy alone or as adjuvant to therapy with curative intent for early nonmetastatic prostate cancer: 5.3-year median followup from the Scandinavian Prostate Cancer Group Study Number 6". The Journal of Urology. 172 (5 Pt 1): 1871–6. doi:10.1097/01.ju.0000139719.99825.54. PMID15540741.
^Iversen P, Johansson JE, Lodding P, Kylmälä T, Lundmo P, Klarskov P, Tammela TL, Tasdemir I, Morris T, Armstrong J (2006). "Bicalutamide 150 mg in addition to standard care for patients with early non-metastatic prostate cancer: updated results from the Scandinavian Prostate Cancer Period Group-6 Study after a median follow-up period of 7.1 years". Scandinavian Journal of Urology and Nephrology. 40 (6): 441–52. doi:10.1080/00365590601017329. PMID17130095. S2CID25862814.
^ abTrüeb RM, Luu NC, Uribe NC, Régnier A (December 2022). "Comment on: Bicalutamide and the new perspectives for female pattern hair loss treatment: What dermatologists should know". J Cosmet Dermatol. 21 (12): 7200–7201. doi:10.1111/jocd.14936. PMID35332669. S2CID247677549. Indeed, due to the minimal biological importance of androgens in women, the adverse effects of bicalutamide are few. And yet, bicalutamide has been associated with elevated liver enzymes, and as of 2021, there have been 10 case reports of liver toxicity associated with bicalutamide, with fatality occurring in 2 cases.2
^Masago T, Watanabe T, Nemoto R, Motoda K (December 2011). "Interstitial pneumonitis induced by bicalutamide given for prostate cancer". International Journal of Clinical Oncology. 16 (6): 763–5. doi:10.1007/s10147-011-0239-x. PMID21537882. S2CID24068787.
^Daba MH, El-Tahir KE, Al-Arifi MN, Gubara OA (June 2004). "Drug-induced pulmonary fibrosis". Saudi Medical Journal. 25 (6): 700–6. PMID15195196.
^Thole Z, Manso G, Salgueiro E, Revuelta P, Hidalgo A (2004). "Hepatotoxicity induced by antiandrogens: a review of the literature". Urologia Internationalis. 73 (4): 289–95. doi:10.1159/000081585. PMID15604569. S2CID24799765.
^Ricci F, Buzzatti G, Rubagotti A, Boccardo F (November 2014). "Safety of antiandrogen therapy for treating prostate cancer". Expert Opinion on Drug Safety. 13 (11): 1483–99. doi:10.1517/14740338.2014.966686. PMID25270521. S2CID207488100.
^Boccardo F (2000). "Hormone therapy of prostate cancer: is there a role for antiandrogen monotherapy?". Crit. Rev. Oncol. Hematol. 35 (2): 121–32. doi:10.1016/s1040-8428(00)00051-2. PMID10936469.
^Thole Z, Manso G, Salgueiro E, Revuelta P, Hidalgo A (2004). "Hepatotoxicity induced by antiandrogens: a review of the literature". Urol. Int. 73 (4): 289–95. doi:10.1159/000081585. PMID15604569. S2CID24799765.
^Bennett CL, Raisch DW, Sartor O (October 2002). "Pneumonitis associated with nonsteroidal antiandrogens: presumptive evidence of a class effect". Annals of Internal Medicine. 137 (7): 625. doi:10.7326/0003-4819-137-7-200210010-00029. PMID12353966. An estimated 0.77% of the 6,480 nilutamide-treated patients, 0.04% of the 41,700 flutamide-treated patients, and 0.01% of the 86,800 bicalutamide-treated patients developed pneumonitis during the study period.
^Foster WR, Car BD, Shi H, Levesque PC, Obermeier MT, Gan J, Arezzo JC, Powlin SS, Dinchuk JE, Balog A, Salvati ME, Attar RM, Gottardis MM (2011). "Drug safety is a barrier to the discovery and development of new androgen receptor antagonists". Prostate. 71 (5): 480–8. doi:10.1002/pros.21263. PMID20878947. S2CID24620044.
^Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, Iversen P, Bhattacharya S, Carles J, Chowdhury S, Davis ID, de Bono JS, Evans CP, Fizazi K, Joshua AM, Kim CS, Kimura G, Mainwaring P, Mansbach H, Miller K, Noonberg SB, Perabo F, Phung D, Saad F, Scher HI, Taplin ME, Venner PM, Tombal B (2014). "Enzalutamide in metastatic prostate cancer before chemotherapy". N. Engl. J. Med. 371 (5): 424–33. doi:10.1056/NEJMoa1405095. PMC4418931. PMID24881730.
^Furr BJ, Tucker H (1996). "The preclinical development of bicalutamide: pharmacodynamics and mechanism of action". Urology. 47 (1A Suppl): 13–25, discussion 29–32. doi:10.1016/S0090-4295(96)80003-3. PMID8560673.
^Greenblatt DJ, Koch-Weser J (July 1973). "Adverse reactions to spironolactone. A report from the Boston Collaborative Drug Surveillance Program". JAMA. 225 (1): 40–3. doi:10.1001/jama.1973.03220280028007. PMID4740303.
^Bahceci M, Tuzcu A, Canoruc N, Tuzun Y, Kidir V, Aslan C (2004). "Serum C-reactive protein (CRP) levels and insulin resistance in non-obese women with polycystic ovarian syndrome, and effect of bicalutamide on hirsutism, CRP levels and insulin resistance". Hormone Research. 62 (6): 283–7. doi:10.1159/000081973 (inactive 2 December 2024). PMID15542929. S2CID46261843.{{cite journal}}: CS1 maint: DOI inactive as of December 2024 (link)
^Genrx (1999). 1999 Mosby's GenRx. Mosby. ISBN978-0-323-00625-5. A 79-year-old man attempted suicide by ingesting 13g of nilutamide (i.e., 43 times the maximum recommended dose). Despite immediate gastric lavage and oral administration of activated charcoal, plasma nilutamide levels peaked at 6 times the normal range 2 hours after ingestion. There were no clinical signs or symptoms or changes in parameters such as transaminases or chest x-ray. Maintenance treatment (150 mg/day) was resumed 30 days later.
^ abcdefghiWeber GF (22 July 2015). Molecular Therapies of Cancer. Springer. pp. 318–. ISBN978-3-319-13278-5. Compared to flutamide and nilutamide, bicalutamide has a 2-fold increased affinity for the Androgen Receptor, a longer half-life, and substantially reduced toxicities. Based on a more favorable safety profile relative to flutamide, bicalutamide is indicated for use in combination therapy with a Gonadotropin Releasing Hormone analog for the treatment of advanced metastatic prostate carcinoma.
^Mosby's GenRx: A Comprehensive Reference for Generic and Brand Prescription Drugs. Mosby. 2001. p. 290. ISBN978-0-323-00629-3. In vitro studies have shown bicalutamide can displace coumarin anticoagulants, such as warfarin, from their protein-binding sites. It is recommended that if bicalutamide is started in patients already receiving coumarin anticoagulants, prothrombin times should be closely monitored and adjustment of the anticoagulant dose may be necessary.
^Furr BK (1997). "Relative potencies of flutamide and 'Casodex'". Endocrine-Related Cancer. 4 (2): 197–202. doi:10.1677/erc.0.0040197 (inactive 1 November 2024). ISSN1351-0088.{{cite journal}}: CS1 maint: DOI inactive as of November 2024 (link)
^Furr BJ (1996). "The development of Casodex (bicalutamide): preclinical studies". European Urology. 29 (Suppl 2): 83–95. doi:10.1159/000473846. PMID8717469.
^ abcdDenis L, Mahler C (January 1996). "Pharmacodynamics and pharmacokinetics of bicalutamide: defining an active dosing regimen". Urology. 47 (1A Suppl): 26–8, discussion 29–32. doi:10.1016/S0090-4295(96)80004-5. PMID8560674.
^Eri LM, Haug E, Tveter KJ (March 1995). "Effects on the endocrine system of long-term treatment with the non-steroidal anti-androgen Casodex in patients with benign prostatic hyperplasia". British Journal of Urology. 75 (3): 335–40. doi:10.1111/j.1464-410X.1995.tb07345.x. PMID7537602.
^ abBouchard P, Caraty A (15 November 1993). GnRH, GnRH Analogs, Gonadotropins and Gonadal Peptides. CRC Press. pp. 455–456. ISBN978-0-203-09205-7. [...] when male levels of androgens are achieved in plasma, their effects on gonadotropin secretion are similar in women and men. [...] administration of flutamide in a group of normally-cycling women produced a clinical improvement of acne and hirsutism without any significant hormonal change. [...] All these data emphasize that physiological levels of androgens have no action on the regulation of gonadotropins in normal women. [...] Androgens do not directly play a role in gonadotropin regulation [in women].
^Asscheman H, Gooren LJ, Peereboom-Wynia JD (1989). "Reduction in undesired sexual hair growth with anandron in male-to-female transsexuals—experiences with a novel androgen receptor blocker". Clinical and Experimental Dermatology. 14 (5): 361–3. doi:10.1111/j.1365-2230.1989.tb02585.x. PMID2612040. S2CID45303518.
^Rao BR, de Voogt HJ, Geldof AA, Gooren LJ, Bouman FG (1988). "Merits and considerations in the use of anti-androgen". Journal of Steroid Biochemistry. 31 (4B): 731–7. doi:10.1016/0022-4731(88)90024-6. PMID3143862.
^ abWibowo E, Schellhammer P, Wassersug RJ (January 2011). "Role of estrogen in normal male function: clinical implications for patients with prostate cancer on androgen deprivation therapy". The Journal of Urology. 185 (1): 17–23. doi:10.1016/j.juro.2010.08.094. PMID21074215.
^ abMotofei IG, Rowland DL, Popa F, Kreienkamp D, Paunica S (July 2011). "Preliminary study with bicalutamide in heterosexual and homosexual patients with prostate cancer: a possible implication of androgens in male homosexual arousal". BJU International. 108 (1): 110–5. doi:10.1111/j.1464-410X.2010.09764.x. PMID20955264. S2CID45482984.
^ abWibowo E, Wassersug RJ (September 2013). "The effect of estrogen on the sexual interest of castrated males: Implications to prostate cancer patients on androgen-deprivation therapy". Critical Reviews in Oncology/Hematology. 87 (3): 224–38. doi:10.1016/j.critrevonc.2013.01.006. PMID23484454.
^Huang Q, Zhu H, Fischer DF, Zhou JN (June 2008). "An estrogenic effect of 5alpha-androstane-3beta, 17beta-diol on the behavioral response to stress and on CRH regulation". Neuropharmacology. 54 (8): 1233–8. doi:10.1016/j.neuropharm.2008.03.016. PMID18457850. S2CID9052079.
^Morgante E, Gradini R, Realacci M, Sale P, D'Eramo G, Perrone GA, Cardillo MR, Petrangeli E, Russo M, Di Silverio F (March 2001). "Effects of long-term treatment with the anti-androgen bicalutamide on human testis: an ultrastructural and morphometric study". Histopathology. 38 (3): 195–201. doi:10.1046/j.1365-2559.2001.01077.x. hdl:11573/387981. PMID11260298. S2CID36892099.
^ abJones CA, Reiter L, Greenblatt E (2016). "Fertility preservation in transgender patients". International Journal of Transgenderism. 17 (2): 76–82. doi:10.1080/15532739.2016.1153992. ISSN1553-2739. S2CID58849546. Traditionally, patients have been advised to cryopreserve sperm prior to starting cross-sex hormone therapy as there is a potential for a decline in sperm motility with high-dose estrogen therapy over time (Lubbert et al., 1992). However, this decline in fertility due to estrogen therapy is controversial due to limited studies.
^ abPayne AH, Hardy MP (28 October 2007). The Leydig Cell in Health and Disease. Springer Science & Business Media. pp. 422–431. ISBN978-1-59745-453-7. Estrogens are highly efficient inhibitors of the hypothalamic-hypophyseal-testicular axis (212–214). Aside from their negative feedback action at the level of the hypothalamus and pituitary, direct inhibitory effects on the testis are likely (215,216). [...] The histology of the testes [with estrogen treatment] showed disorganization of the seminiferous tubules, vacuolization and absence of lumen, and compartmentalization of spermatogenesis.
^ abSalam MA (2003). Principles & Practice of Urology: A Comprehensive Text. Universal-Publishers. pp. 684–. ISBN978-1-58112-412-5. Estrogens act primarily through negative feedback at the hypothalamic-pituitary level to reduce LH secretion and testicular androgen synthesis. [...] Interestingly, if the treatment with estrogens is discontinued after 3 yr. of uninterrupted exposure, serum testosterone may remain at castration levels for up to another 3 yr. This prolonged suppression is thought to result from a direct effect of estrogens on the Leydig cells.
^ abFoster WR, Car BD, Shi H, Levesque PC, Obermeier MT, Gan J, Arezzo JC, Powlin SS, Dinchuk JE, Balog A, Salvati ME, Attar RM, Gottardis MM (April 2011). "Drug safety is a barrier to the discovery and development of new androgen receptor antagonists". The Prostate. 71 (5): 480–8. doi:10.1002/pros.21263. PMID20878947. S2CID24620044.
^Blackledge GR (1996). "Clinical progress with a new antiandrogen, Casodex (bicalutamide)". Eur. Urol. 29 (Suppl 2): 96–104. doi:10.1159/000473847. PMID8717470.
^Furr BJ (1989). ""Casodex" (ICI 176,334)--a new, pure, peripherally-selective anti-androgen: preclinical studies". Hormone Research. 32 (Suppl 1): 69–76. doi:10.1159/000181315 (inactive 11 November 2024). PMID2533159.{{cite journal}}: CS1 maint: DOI inactive as of November 2024 (link)
^Furr BJ, Valcaccia B, Curry B, Woodburn JR, Chesterson G, Tucker H (June 1987). "ICI 176,334: a novel non-steroidal, peripherally selective antiandrogen". The Journal of Endocrinology. 113 (3): R7-9. doi:10.1677/joe.0.113R007. PMID3625091.
^Soloway MS, Schellhammer PF, Smith JA, Chodak GW, Vogelzang NJ, Kennealey GT (December 1995). "Bicalutamide in the treatment of advanced prostatic carcinoma: a phase II noncomparative multicenter trial evaluating safety, efficacy and long-term endocrine effects of monotherapy". The Journal of Urology. 154 (6): 2110–4. doi:10.1016/S0022-5347(01)66709-0. PMID7500470.
^Mason M (August 2006). "What implications do the tolerability profiles of antiandrogens and other commonly used prostate cancer treatments have on patient care?". Journal of Cancer Research and Clinical Oncology. 132 (Suppl 1): S27-35. doi:10.1007/s00432-006-0134-4. PMID16896883. S2CID19685819.
^Fradet Y (February 2004). "Bicalutamide (Casodex) in the treatment of prostate cancer". Expert Review of Anticancer Therapy. 4 (1): 37–48. doi:10.1586/14737140.4.1.37. PMID14748655. S2CID34153031. In contrast, the incidence of diarrhea was comparable between the bicalutamide and placebo groups (6.3 vs. 6.4%, respectively) in the EPC program [71].
^Sharma K, Pawar GV, Giri S, Rajagopal S, Mullangi R (2012). "Development and validation of a highly sensitive LC-MS/MS-ESI method for the determination of bicalutamide in mouse plasma: application to a pharmacokinetic study". Biomedical Chromatography. 26 (12): 1589–95. doi:10.1002/bmc.2736. PMID22495777.
^Anderson PO, Knoben JE, Troutman WG (22 August 2001). Handbook of Clinical Drug Data. Canadian Medical Association Journal. Vol. 128. McGraw Hill Professional. p. 245. ISBN978-0-07-138942-6. PMC1875767. PMID20313924. With an oral dose of 50 mg/day, bicalutamide attains a peak serum level of 8.9 mg/L (21 μmol/L) 31 hr after a dose at steady state. CI of (R)-bicalutamide is 0.32 L/hr. The active (R)-enantiomer of bicalutamide is oxidized to an inactive metabolite, which, like the inactive (S)-enantiomer, is glucuronidated and cleared rapidly by elimination in the urine and feces.165
^ abcdeMohler ML, Bohl CE, Jones A, Coss CC, Narayanan R, He Y, Hwang DJ, Dalton JT, Miller DD (June 2009). "Nonsteroidal selective androgen receptor modulators (SARMs): dissociating the anabolic and androgenic activities of the androgen receptor for therapeutic benefit". Journal of Medicinal Chemistry. 52 (12): 3597–617. doi:10.1021/jm900280m. PMID19432422. [C]linically relevant antiandrogens currently are nonsteroidal anilide derivatives. Antiandrogens used for prostate cancer include the monoarylpropionamide flutamide (1) (a prodrug of hydroxyflutamide (2)),29–31 the hydantoin nilutamide(3),32–34 and the diarylpropionamide bicalutamide (4) (Chart1).35–37
^ abcSegal S, Narayanan R, Dalton JT (April 2006). "Therapeutic potential of the SARMs: revisiting the androgen receptor for drug discovery". Expert Opinion on Investigational Drugs. 15 (4): 377–87. doi:10.1517/13543784.15.4.377. PMID16548787. S2CID31787187. Structural modifications of bicalutamide led to the discovery of the first nonsteroidal androgens (the aryl propionamides) in 1998. Lead compounds in this class (denoted S1 and S4 in published literature) not only bind to the AR with high affinity (low nanomolar range), but also demonstrate tissue selectivity in animal models [46,50].
^ abcdParent EE, Dence CS, Jenks C, Sharp TL, Welch MJ, Katzenellenbogen JA (2007). "Synthesis and biological evaluation of [18F]bicalutamide, 4-[76Br]bromobicalutamide, and 4-[76Br]bromo-thiobicalutamide as non-steroidal androgens for prostate cancer imaging". J. Med. Chem. 50 (5): 1028–40. doi:10.1021/jm060847r. PMID17328524.
^ abde Jesus Cortez F, Nguyen P, Truillet C, Tian B, Kuchenbecker KM, Evans MJ, Webb P, Jacobson MP, Fletterick RJ, England PM (2017). "Development of 5N-Bicalutamide, a High-Affinity Reversible Covalent Antiandrogen". ACS Chem. Biol. 12 (12): 2934–2939. doi:10.1021/acschembio.7b00702. PMID28981251. S2CID24974359.
^US Patent 10053433B2, England, Pamela M.; Fletterick, R. J. & Kuchenbecker, K. et al., published 2016
^ abcTucker H, Crook JW, Chesterson GJ (1988). "Nonsteroidal antiandrogens. Synthesis and structure-activity relationships of 3-substituted derivatives of 2-hydroxypropionanilides". Journal of Medicinal Chemistry. 31 (5): 954–9. doi:10.1021/jm00400a011. PMID3361581.
^James KD, Ekwuribe NN (2002). "A Two-step Synthesis of the Anti-cancer Drug (R,S)-Bicalutamide". Synthesis. 2002 (7): 850–2. doi:10.1055/s-2002-28508.
^Chand M, Shukla AK (2012). Novel Synthesis of Bicalutamide Drug Substance and their Impurities using Imidazolium Type of Ionic Liquid (Report). doi:10.2139/ssrn.2160199. SSRN2160199.
^Diamanti-Kandarakis E (September 1999). "Current aspects of antiandrogen therapy in women". Current Pharmaceutical Design. 5 (9): 707–23. doi:10.2174/1381612805666230111201150. PMID10495361. Archived from the original on 10 January 2023. Retrieved 27 September 2016. Several trials demonstrated complete clearing of acne with flutamide [62,77]. Flutamide used in combination with an [oral contraceptive], at a dose of 500mg/d, flutamide caused a dramatic decrease (80%) in total acne, seborrhea and hair loss score after only 3 months of therapy [53]. When used as a monotherapy in lean and obese PCOS, it significantly improves the signs of hyperandrogenism, hirsutism and particularly acne [48]. [...] flutamide 500mg/d combined with an [oral contraceptive] caused an increase in cosmetically acceptable hair density, in sex of seven women suffering from diffuse androgenetic alopecia [53].
^Furr BJ, Valcaccia B, Curry B, Woodburn JR, Chesterson G, Tucker H (June 1987). "ICI 176,334: a novel non-steroidal, peripherally selective antiandrogen". The Journal of Endocrinology. 113 (3): R7-9. doi:10.1677/joe.0.113r007. PMID3625091.
^Newling DW (1990). "The response of advanced prostatic cancer to a new non-steroidal antiandrogen: results of a multicenter open phase II study of Casodex. European/Australian Co-operative Group". European Urology. 18 (Suppl 3): 18–21. doi:10.1159/000463973. PMID2094607.
^Chaurasiya A, Singh AK, Upadhyay SC, Asati D, Ahmad FJ, Mukherjee R, Khar (2012). "Lipidic Nanocarrier for Oral Bioavailability Enhancement of an Anticancer Agent: Formulation Design and Evaluation". Advanced Science Letters. 11 (1): 43–52. doi:10.1166/asl.2012.2170. ISSN1936-6612.
^Klotz L (May 2006). "Combined androgen blockade: an update". The Urologic Clinics of North America. 33 (2): 161–6, v–vi. doi:10.1016/j.ucl.2005.12.001. PMID16631454.
^Kolvenbag GJ, Iversen P, Newling DW (2001). "Antiandrogen monotherapy: a new form of treatment for patients with prostate cancer". Urology. 58 (2 Suppl 1): 16–23. doi:10.1016/s0090-4295(01)01237-7. PMID11502439.
^Jasmin C, Capanna R, Coia L, Coleman R, Saillant G (27 September 2005). Textbook of Bone Metastases. John Wiley & Sons. pp. 493–. ISBN978-0-470-01160-7. Archived from the original on 14 January 2023. Retrieved 27 September 2016.
^Bono AV (2004). "Overview of Current Treatment Strategies in Prostate Cancer". European Urology Supplements. 3 (1): 2–7. doi:10.1016/j.eursup.2003.12.002. The Canadian Health Authorities have withdrawn the approval for antiandrogen monotherapy with bicalutamide for the treatment of localised prostate cancer [5]. Several European countries have also withdrawn approval for bicalutamide for this indication.
^Emans SJ, Laufer MR (5 January 2012). Emans, Laufer, Goldstein's Pediatric and Adolescent Gynecology. Lippincott Williams & Wilkins. pp. 365–. ISBN978-1-4511-5406-1. Archived from the original on 16 May 2016. Therapy with GnRH analogs is expensive and requires intramuscular injections of depot formulations, the insert of a subcutaneous implant yearly, or, much less commonly, daily subcutaneous injections.
^Wang LG, Mencher SK, McCarron JP, Ferrari AC (2004). "The biological basis for the use of an anti-androgen and a 5-alpha-reductase inhibitor in the treatment of recurrent prostate cancer: Case report and review". Oncology Reports. 11 (6): 1325–9. doi:10.3892/or.11.6.1325. PMID15138573.
^Merrick GS, Butler WM, Wallner KE, Galbreath RW, Allen ZA, Kurko B (2006). "Efficacy of neoadjuvant bicalutamide and dutasteride as a cytoreductive regimen before prostate brachytherapy". Urology. 68 (1): 116–20. doi:10.1016/j.urology.2006.01.061. PMID16844453.
^Sartor O, Gomella LG, Gagnier P, Melich K, Dann R (2009). "Dutasteride and bicalutamide in patients with hormone-refractory prostate cancer: the Therapy Assessed by Rising PSA (TARP) study rationale and design". The Canadian Journal of Urology. 16 (5): 4806–12. PMID19796455.
^Chu FM, Sartor O, Gomella L, Rudo T, Somerville MC, Hereghty B, Manyak MJ (2015). "A randomised, double-blind study comparing the addition of bicalutamide with or without dutasteride to GnRH analogue therapy in men with non-metastatic castrate-resistant prostate cancer". European Journal of Cancer. 51 (12): 1555–69. doi:10.1016/j.ejca.2015.04.028. PMID26048455.
^Gaudet M, Vigneault É, Foster W, Meyer F, Martin AG (2016). "Randomized non-inferiority trial of Bicalutamide and Dutasteride versus LHRH agonists for prostate volume reduction prior to I-125 permanent implant brachytherapy for prostate cancer". Radiotherapy and Oncology. 118 (1): 141–7. doi:10.1016/j.radonc.2015.11.022. PMID26702991.
^ abcdLepor H (1993). "Medical therapy for benign prostatic hyperplasia". Urology. 42 (5): 483–501. doi:10.1016/0090-4295(93)90258-c. PMID7694413. The clinically significant adverse events reported in the casodex group included breast tenderness (93%), breast enlargement (54%), and sexual dysfunction (60%). In none of the patients in the placebo group did any of these adverse events develop. None of the subjects discontinued therapy owing to an adverse event.
^Kenny B, Ballard S, Blagg J, Fox D (1997). "Pharmacological options in the treatment of benign prostatic hyperplasia". J. Med. Chem. 40 (9): 1293–315. doi:10.1021/jm960697s. PMID9135028.
^Fox JG, Marini RP (26 March 2014). Biology and Diseases of the Ferret. Wiley. p. 980. ISBN978-1-118-78273-6. Other agents have been proposed for medical management of [adrenal-associated endocrinopathy] but have not been studied. Possibly medications include the androgen receptor blockers flutamide and bicalutamide, the anti-androgen finasteride, estrogen-inhibiting anastrozole, and another GnRH analog, goserelin. [...] None of these drugs have been tested in controlled clinical trials in ferrets.
Blackledge GR (1996). "Clinical progress with a new antiandrogen, Casodex (bicalutamide)". European Urology. 29 (Suppl 2): 96–104. doi:10.1159/000473847. PMID8717470.
Furr BJ, Tucker H (January 1996). "The preclinical development of bicalutamide: pharmacodynamics and mechanism of action". Urology. 47 (1A Suppl): 13–25, discussion 29–32. doi:10.1016/S0090-4295(96)80003-3. PMID8560673.
Kolvenbag GJ, Blackledge GR (January 1996). "Worldwide activity and safety of bicalutamide: a summary review". Urology. 47 (1A Suppl): 70–9, discussion 80–4. doi:10.1016/s0090-4295(96)80012-4. PMID8560681.
Schellhammer PF, Davis JW (March 2004). "An evaluation of bicalutamide in the treatment of prostate cancer". Clinical Prostate Cancer. 2 (4): 213–9. doi:10.3816/CGC.2004.n.002. PMID15072604.
Tucker H, Crook JW, Chesterson GJ (1988). "Nonsteroidal antiandrogens. Synthesis and structure-activity relationships of 3-substituted derivatives of 2-hydroxypropionanilides". J. Med. Chem. 31 (5): 954–9. doi:10.1021/jm00400a011. PMID3361581.
This article needs additional citations for verification. Please help improve this article by adding citations to reliable sources. Unsourced material may be challenged and removed.Find sources: List of Hindi films of 1998 – news · newspapers · books · scholar · JSTOR (January 2019) (Learn how and when to remove this template message) Hindi cinema 1920s 1920 1921 1922 1923 19241925 1926 1927 1928 1929 1930s 1930 1931 1932 1933 19341935 1936 1937 1938 1939…
Resolusi 6Dewan Keamanan PBBBendera Perserikatan Bangsa-BangsaTanggal17 Mei 1946Sidang no.42KodeS/RES/6 (Dokumen)TopikPendaftaran keanggotaanRingkasan hasil11 mendukungTidak ada menentangTidak ada abstainHasilDiadopsiKomposisi Dewan KeamananAnggota tetap Tiongkok (ROC) Prancis Britania Raya Amerika Serikat Uni SovietAnggota tidak tetap Australia Brasil Mesir Meksiko Belanda Polandia Resolusi 6 Dewan Keamanan Perserikatan Bangsa-Ban…
Highest peak in Hong Kong Tai Mo ShanTai Mo Shan, viewed from Tai To Yan in April 2008Highest pointElevation957 m (3,140 ft)Hong Kong Principal Datum Coordinates22°24′42.52″N 114°7′23.32″E / 22.4118111°N 114.1231444°E / 22.4118111; 114.1231444NamingNative nameTai Mo Shan (English)大帽山 (Cantonese)GeographyTai Mo ShanLocation of Tai Mo Shan in Hong Kong LocationCentre of the New Territories, Hong Kong Tai Mo Shan Road, and Tai …
العلاقات النمساوية الكوستاريكية النمسا كوستاريكا النمسا كوستاريكا تعديل مصدري - تعديل العلاقات النمساوية الكوستاريكية هي العلاقات الثنائية التي تجمع بين النمسا وكوستاريكا.[1][2][3][4][5] مقارنة بين البلدين هذه مقارنة عامة ومرجعية للدولتي�…
Cultural and historical region in France Lothringen redirects here. For other uses, see Lorraine (disambiguation), Lauren (disambiguation), and Lothringen (disambiguation). This article needs additional citations for verification. Please help improve this article by adding citations to reliable sources. Unsourced material may be challenged and removed.Find sources: Lorraine – news · newspapers · books · scholar · JSTOR (August 2022) (Learn how and when to…
This article does not cite any sources. Please help improve this article by adding citations to reliable sources. Unsourced material may be challenged and removed.Find sources: Azadegan Expressway – news · newspapers · books · scholar · JSTOR (June 2019) (Learn how and when to remove this template message) Azadegan Expresswayبزرگراه آزادگانRoute informationLength36.4 km (22.6 mi)Major junctionsEast endBasij Interchange Ba…
Ferdinando III d'AsburgoFrans Luycx, ritratto dell'imperatore Ferdinando III, 1637 circa; Kunsthistorisches MuseumImperatore Eletto dei RomaniStemma In carica15 febbraio 1637 –2 aprile 1657 Incoronazione18 novembre 1637 PredecessoreFerdinando II SuccessoreLeopoldo I Re d'Ungheria e CroaziaRe di BoemiaIn carica15 febbraio 1637 –2 aprile 1657 Incoronazione8 dicembre 1625 (Ungheria)21 novembre 1627 (Boemia) PredecessoreFerdinando II SuccessoreLeopoldo I Altri titoliRe in Germani…
This article needs additional citations for verification. Please help improve this article by adding citations to reliable sources. Unsourced material may be challenged and removed.Find sources: Miami International Mall – news · newspapers · books · scholar · JSTOR (February 2018) (Learn how and when to remove this template message) Shopping mall in Florida, United StatesMiami International MallEast entrance between JCPenney and Elev8LocationDoral, Florid…
Roman Catholic parish church in New York City, United States Church of St. ElizabethGeneral informationArchitectural styleGothic RevivalTown or cityNew York CityCountryUnited StatesCompleted1913 (rectory)[1]1929 (for present church)ClientRoman Catholic Archdiocese of New YorkTechnical detailsStructural systemMasonry stoneDesign and constructionArchitect(s)Edward Lee Young of 12 East 30th Street[1]WebsiteSt. Elizabeth's Catholic Church, Manhattan Church of St. Elizabeth is a Roman…
This article needs additional citations for verification. Please help improve this article by adding citations to reliable sources. Unsourced material may be challenged and removed.Find sources: Whitton Park – news · newspapers · books · scholar · JSTOR (January 2017) (Learn how and when to remove this template message) Whitton Park was a country house in the village of Whitton in Twickenham, Middlesex. It was demolished in the 1840s and gradually replace…
Madhya Pradesh Legislative Assembly Election 2008 ← 2003 27 November 2008 2013 → All 230 assembly constituencies116 seats needed for a majorityRegistered36,266,969Turnout69.63% 2.38% Majority party Minority party Third party Leader Shivraj Singh Chouhan Suresh Pachouri Mayawati Party BJP INC BSP Leader's seat Budhni Did not contest Did not contest Last election 173 38 2 Seats won 143 71 7 Seat change 30 33 5 Popular vote 9,493,641 8,17…
Lockheed L-749 ConstellationTrans World Airlines L-749ATipePesawat terbangPerancangClarence Kelly JohnsonTerbang perdana14 Maret 1947[1]Diperkenalkan18 April 1947Dipensiunkan1993StatusDipensiunkanPengguna utamaTrans World AirlinesPengguna lainAir France KLMEastern Air LinesTahun produksi1947 - 1951[2][3]Jumlah produksi119Acuan dasarL-649 ConstellationVarianC-121 Constellation PO-1W/WV-1 Constellation Lockheed L-749 Constellation adalah pesawat pertama dari varian Lockheed…
KI BOIS Area Transit SystemHeadquarters1107 Industrial Road, Stigler, OklahomaAnnual ridership508,053 (2022)[1]DirectorCharla SloanWebsiteOfficial website KI BOIS Area Transit System (KATS) is a rural public transportation organization centered mostly in Southeastern Oklahoma, and specifically in the counties of Adair, Cherokee, Haskell, Latimer, LeFlore, McIntosh, Okfuskee, Okmulgee, Pittsburg, Sequoyah, and Wagoner.[2] It is run by KI BOIS Community Action, Inc., a private, non…
Lowest tier of administration within a sovereign state This article possibly contains original research. Please improve it by verifying the claims made and adding inline citations. Statements consisting only of original research should be removed. (January 2011) (Learn how and when to remove this message) Part of the Politics seriesBasic forms of government List of forms of government List of countries by system of government Source of power Democracy (rule by many) Demarchy Direct Liberal Repre…
BBC documentary film about the Monty Python team The PythonsTitle cardGenreDocumentaryStarringGraham ChapmanJohn CleeseTerry GilliamEric IdleTerry JonesMichael PalinNarrated byIain Johnstone[1]Country of originUnited KingdomOriginal languageEnglishProductionProducerIain Johnstone[1]EditorHeather SmallCamera setupJohn WalkerRunning time50 minutesOriginal releaseNetworkBBC 1Release20 June 1979 (1979-06-20)[1] The Pythons is a BBC documentary film about the Mo…
Berikut adalah Daftar perguruan tinggi swasta di Kalimantan Selatan, yang pembinaannya berada di bawah Kementerian Pendidikan dan Kebudayaan Republik Indonesia dan Perguruan Tinggi Swasta Keagamaan, yang pembinaannya berada di bawah Kementerian Agama. Daftar ini tidak termasuk Perguruan Tinggi Kedinasan yang pembinaannya berada dibawah masing-masing kementerian/lembaga. Akademi Akademi Farmasi ISFI, Banjarmasin Akademi Kebidanan Abdi Persada Banjarmasin Akademi Kebidanan Banjarbaru, Banjarbaru A…
В Википедии есть статьи о других людях с такой фамилией, см. Арсеньев. Илья Александрович Арсеньев Портрет 1862 г. Дата рождения 1820(1820) Место рождения Москва Дата смерти 16 (28) февраля 1887(1887-02-28) Место смерти Санкт-Петербург Подданство Российская империя Род деятельн�…
Cet article est une ébauche concernant la bière et le Viêt Nam. Vous pouvez partager vos connaissances en l’améliorant (comment ?) selon les recommandations des projets correspondants. Si ce bandeau n'est plus pertinent, retirez-le. Cliquez ici pour en savoir plus. Cet article présente des problèmes à corriger. Vous pouvez aider à l'améliorer ou bien discuter des problèmes sur sa page de discussion. Il ne cite pas suffisamment ses sources. Vous pouvez indiquer les passages à so…
Hôpital San SalvadourGéographiePays FranceDivision territoriale française France métropolitaineRégion Provence-Alpes-Côte d'AzurDépartement français VarPartie de Assistance publique – Hôpitaux de Paris, structures de soin de l'AP-HP (hors GH) (d)Coordonnées 43° 05′ 05″ N, 6° 06′ 34″ EFonctionnementStatut HôpitalIdentifiantsSite web www.aphp.fr/contenu/hopital-san-salvadour-2modifier - modifier le code - modifier Wikidata L'hôpital San S…


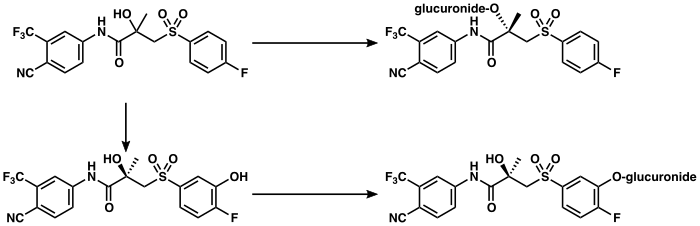



















")




")


")
